Original Article Comparative Study of Functional Outcome of Idiopathic Congenital Talipes Equinovarus Treated between Ponseti Technique and Accelerated Ponseti Technique using Pirani Score
Ponseti Technique and Accelerated Ponseti Technique for Idiopathic CTEV
Keywords:
Accelerated Ponseti method, congenital talipes equinovarus, Ponseti methodAbstract
Background and Objectives: Congenital talipes equinovarus (CTEV), also known as clubfoot, is one of the most prevalent
birth disorders affecting the musculoskeletal system and affects one in 1000 live births. The tried-and-true Ponseti method of
therapy entails weekly adjustment of the deformity followed by a long-leg cast. Modified accelerated treatment protocols were
designed to reduce the total duration of treatment. This study was conducted to compare the efficacy of accelerated Ponseti
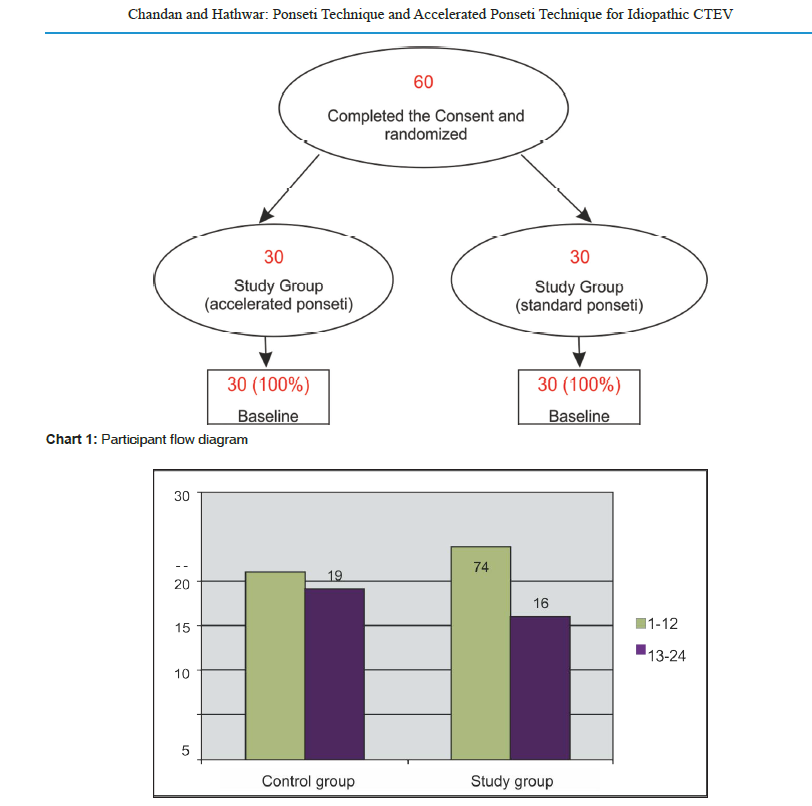
method versus standard Ponseti method. Methods: A randomized controlled study was conducted with participants randomized
to two groups-Study group and Control groups. All feet were scored using Pirani score, recorded by an independent assessor at
each visit. Plaster treatment was continued until clinical correction achieved. Results: The study had 100% subject retention in
both the groups from baseline to follow-up. The current study had comparable demographic distribution between the groups.
Accelerated Ponseti technique has relatively shorter duration of manipulation compared to the standard Ponseti technique.
Total number of casts used is not significantly different for accelerated Ponseti technique compared to the standard Ponseti
technique. Accelerated Ponseti technique for club foot management was found to be equally effective compared to the standard
Ponseti technique in managing idiopathic CTEV assessed by Pirani scoring. Interpretation and Conclusion: According to
the best evidence synthesis, no evidence exists to support the use of a cast change interval of 1 week. It can be concluded that
the accelerated versions of the Ponseti method can safely be used in the treatment of clubfoot without risking any significant
increase in the required number of casts.
References
REFERENCES
Roye Jr DP, Roye BD. Idiopathic congenital talipes
equinovarus. J Am Acad Orthop Surg 2002;10:239-48.
Kite JH. Nonoperative treatment of congenital clubfoot. Clin
Orthop 1972;84:29-38.
Ikeda K. Conservative treatment of idiopathic clubfoot. J
Pediatr Orthop 1992;12:217-23.
Ponseti IV, Smoley EN. Congenital clubfoot-the results of
treatment. J Bone Joint Surg 45:134-41.
van Bosse HJ. Ponseti treatment for clubfeet: An international
perspective. Curr Opin Pediatr 2011;23:41-5.
Morcuende JA, Abbasi D, Dolan LA, Ponseti IV. Results of
an accelerated Ponseti protocol for clubfoot. J Pediatr Orthop
;25:623-6.
Xu RJ. A modified Ponseti method for the treatment of
idiopathic clubfoot: A preliminary report. J Pediatr Orthop
;31:317-9.
Byron‐Scott R, Sharpe P, Hasler C, Cundy P, Hirte C, Chan
A, et al. A South Australian population‐based study of
congenital talipes equinovarus. Paediatr Perinat Epidemiol
;19:227-37.
Maranho DA, Nogueira-Barbosa MH, Simão MN, Volpon JB.
Ultrasonographic evaluation of Achilles tendon repair after
percutaneous sectioning for the correction of congenital
clubfoot residual equinus. J Pediatr Orthop 2009;29:804-10.
Ponseti IV, Ponseti IV. Common errors in the treatment of
congenital clubfoot. Int Orthop 1997;21:137.
Dimeglio A. Classification of talipes equinovarus. In: The
Clubfoot. New York, NY: Springer. 1994. p. 92-3.
Pandey S, Pandey AK. The classification of clubfoot a practical
approach. Foot 2003;13:61-5.
Chu A, Labar AS, Sala DA, van Bosse HJ, Lehman WB.
Clubfoot classification: Correlation with Ponseti cast treatment.
J Pediatr Orthop 2010;30:695-9.
Flynn JM, Donohoe M, Mackenzie WG. An independent
assessment of two clubfoot-classification systems. J Pediatr
Orthop 1998;18:323-7.
Patel DS, Gadhavi M, Patel A, Taral J, Poriya H. Results of
ponseti Method in Congenital Talipes Equino Varus Children
of More Than 1.5 Years of Age.
Herzenberg JE, Radler C, Bor N. Ponseti versus traditional
methods of casting for idiopathic clubfoot. J Pediatr Orthop
;22:517-21.
van Bosse HJ. Ponseti treatment for clubfeet: an international
perspective. Curr Opin Pediatr 2011;23:41-5.
Morcuende JA, Abbasi D, Dolan LA, Ponseti IV. Results of
an accelerated Ponseti protocol for clubfoot. J Pediatr Orthop
;25:623-6.
Elgohary HS, Abulsaad M. Traditional and accelerated Ponseti
technique: A comparative study. Eur J Orthop Surg Traumatol
;25:949-53.
Harshwardhan H, Kumar S. Evaluation of outcome in
idiopathic clubfoot managed by accelerated Ponseti method.
Int J Orthop Sci 2018;4:172-6.
Dutta A, Sipani AK, Kumar P. A comparative study between
standard and accelerated ponseti method in management
of idiopathic congenital talipes equinovarus. Int J Orthop
;5:359-63.
Ahmed J, Shahid S, Alam W, Ahmed A, Hussain H, Akram R,
et al. Outcome of patients suffering from congenital
This
idiopathic club foot: A comparative analysis of using classical
versus accelerated ponseti techniques. J Pak Orthop Assoc
;31:44-7.
Sarrafan N, Nasab SA, Fakoor M, Zakeri A. Short term
outcome of congenital clubfoot treated by Ponseti method. Pak
J Med Sci Q 2012;28:459.
Ibraheem GH, Adegbehingbe OO, Babalola OM, Agaja SB,
Ahmed BA, Olawepo A, et al. Evaluation of an accelerated
Ponseti protocol for the treatment of talipesequinovarus in
Nigeria. East Central Afr J Surg 2017;22:28-38.
Ahmad MN, Ghani A, Nissar SK. Management of Clubfoot
with Accelerated Ponseti Casting Method at Tertiary Care
Hospital, GMC Jammu India
Published
How to Cite
Issue
Section
Copyright (c) 2023 Journal of Bones & Muscles Health

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.